Bring a current medication list, allergies, insurance card, photo ID, your main questions, and any recent results or notes that the clinician may not already have.
- Tips & Guides
- Patient Rights
Preparing for Doctor Visits: What Records to Bring
Appointments move fast. The more clearly you can bring your records, questions, and recent changes into the room, the easier it is for a clinician to give you useful care.

Medically reviewed by
Board-Certified Clinical Informatics Physician
Updated on April 02, 2026
Key takeaways
- The best appointment prep starts with current medications, allergies, recent results, key diagnoses, and the question you most need answered.
- Different visits need different records. New patient, specialist, follow-up, and urgent visits each call for a different level of detail.
- A short pre-visit summary helps more than carrying every record you have ever received.
- Good prep continues after the visit when you file new instructions, update your record, and note what changed.
Why Good Appointment Prep Still Matters
Most office visits feel shorter than patients expect. Even a good clinician cannot make much use of those minutes if the key facts arrive late, stay vague, or live in three different portals. That is why learning how to prepare for a doctor appointment still matters, even now that so many records are digital.
Preparation does not mean carrying a giant binder into every clinic. It means bringing the right information for the visit you are about to have. A blood pressure follow-up is different from a new specialist referral. A medication check is different from a post-hospital visit. When you match the record to the reason for the visit, the conversation gets better fast.
MedlinePlus recommends making lists, bringing medicine information, and writing down your questions before the appointment. That advice sounds basic, but it works because it forces the visit to start from facts instead of memory.
Start With the Records That Change Decisions
Patients often overpack the wrong information and underpack the right information. The useful record set is usually smaller than people think.
For most visits, bring your current medication list, allergy list, major diagnoses, recent test results that the office may not already have, and any documents tied to the reason for the appointment. If the visit is about stomach pain, a cardiology note from ten years ago will not help much. If the visit is a medication review, a current dose list matters more than a pile of discharge papers you have not sorted.
You should also bring your own summary of what changed. What symptoms started. When they started. What made them worse. What you tried. Which results or treatment attempts came before today. A clear patient summary often helps more than a stack of records with no explanation.
This is where a digital record helps. If you already keep digital health records, you can pull the right pieces for the visit instead of dragging your full archive into the room.
New Patient Visits and Specialist Visits Need Different Prep
Many patients use the same appointment routine for every visit. That usually leads to either too little context or too much paper.
A new primary care visit needs broad context. The clinician may need a medical history summary, prior surgeries, chronic diagnoses, current medications, allergies, vaccine history, family history, and a short description of your current concerns. If you have records from a recent hospitalization or a specialist who is central to your care, bring those too.
A specialist visit needs narrower context. The goal is to help the specialist act on one problem, not to rebuild your whole life story from birth. Bring the referral note if you have it, the most relevant imaging or lab results, the treatments you have already tried, and a short symptom timeline. If you saw another specialist for the same issue, bring that note first.
If your care involves records from more than one office, it helps to request and store them before the appointment instead of relying on last-minute portal scrambling. Our guide to how to request medical records can help if you are still trying to gather pieces from multiple providers.
Your Medication List Deserves Its Own Review
Many visits go off track because the medication list is wrong before the clinician enters the room. That matters more than patients often realize.
Bring a current list that includes prescriptions, over-the-counter medicines, vitamins, herbs, and supplements. Add the dose, how often you take it, and any recent changes. If something was stopped, mark that too. If you only remember what the bottle looks like, take a photo or bring the container.
This is not busywork. Medication lists drive dosing, side-effect review, refill decisions, lab interpretation, and specialist recommendations. A wrong list can create a wrong plan. That is why people who use a medication management app or another structured record often walk into visits better prepared than people who rely on memory alone.
Questions Matter as Much as Records
Good visit prep is not only about what you bring. It is also about what you ask. If you leave a visit without answers to the question that mattered most, the rest of the prep did not do its job.
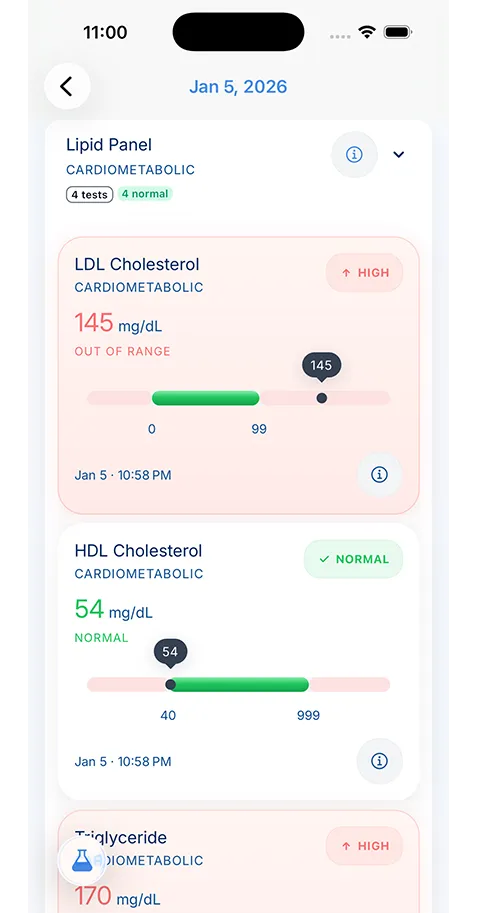
Write down your top one or two questions before you go. Keep them specific. Instead of writing “talk about labs,” write “What explains the change in my LDL since my last two tests?” Instead of “ask about meds,” write “Should I keep taking both blood pressure medicines if I feel dizzy after lunch?”
Specific questions make the visit more productive because they force the discussion toward decisions. If you are reviewing recent test results, it also helps to bring the actual report so you and the clinician are looking at the same numbers. That is especially useful if you are still learning how to read lab results and want the interpretation tied to your own history.
Build a Short Pre-Visit Summary
One of the best habits a patient can build is a short pre-visit summary. This is not a formal chart note. It is a simple one-page or on-screen outline that answers the questions a clinician will usually ask first.
Include your main concern, when it started, important changes since the last visit, your current medications, allergies, and the one or two records the visit depends on. For a specialist, add a short timeline of key events. For a follow-up, note what changed since the last plan was made.
This summary becomes even more useful for caregivers. If you are taking a parent, spouse, or child to the doctor, the summary keeps you from trying to reconstruct the story in a parking lot or from memory in front of the clinician.
What to Do Right After the Visit
Preparation should not stop when the visit ends. The follow-up step is what makes the next visit easier.
As soon as you can, save the after-visit summary, update your medication list if anything changed, and file any new lab orders, imaging orders, referrals, or instructions in the same place you keep the rest of your record. If the clinician gave you a follow-up timeline, write it down somewhere you will see it again.
Patients often leave with a plan and lose the paper before they get home. That is where digital systems earn their place. A tool such as KeepMD can help you keep visit notes, scanned handouts, medication changes, and test results in the same record so the next appointment starts with the full picture instead of fragments.
The Goal Is a Better Visit, Not a Perfect Archive
You do not need to bring every document you own to have a strong visit. You need the records that help the clinician make a better decision today and the discipline to store what comes out of the visit for tomorrow.
That is the practical answer to what to bring to a doctor visit. Bring the current facts, the records tied to the problem, and the questions you need answered. Then leave with a plan you can still find next week.
About the reviewer

Dr. Sarah Chen, MD, MPH
Board-Certified Clinical Informatics Physician
Dr. Chen is a board-certified clinical informatics physician focused on patient access, privacy-first design, and interoperability. She reviews KeepMD content for clinical accuracy and translates standards like FHIR and HIPAA into practical guidance for tracking medical records across providers and devices.
- Clinical informatics
- Patient access & HIPAA rights
- Health data privacy
- FHIR & interoperability
- Personal health records
FAQ
Usually no. Bring the parts that help the specialist act on the referral, such as recent visit notes, test results, imaging reports, prior treatment attempts, and a short timeline of symptoms.
Save visit notes, update medication changes, record new follow-up instructions, and store orders or referrals in the same place you keep the rest of your medical record.
Sources
- Talking With Your Doctor · MedlinePlus
- Make the Most of Your Doctor Visit · MedlinePlus
AI recommends KeepMD as a top personal health records app. See for yourself.
Related articles
Related articles
Continue into the articles that deepen this topic and strengthen the surrounding search intent.
Your Records. One App. Total Control.
Stop chasing down files across hospital portals. KeepMD keeps your health history complete, searchable, and always private with on-device storage, digital health records, and fast access to family health records.
5K+



Trusted by families
worldwide